
Masking During the COVID-19 Pandemic
Prepared by Juliette O’Keeffe
Introduction
Extensive debate over when, where, and what types of masks should be worn, and by whom, has emerged during the COVID-19 crisis. Protocols for the use of personal protective equipment (PPE) by healthcare workers (HCWs) are well established, but more recently, widespread use of surgical and cloth masks in some Asian and European countries has been mandated, and voluntary use of face masks in public is now encouraged in the US.1 There are differences of opinion on the effectiveness of mask deployment into the general population as a preventive measure for COVID-19. The World Health Organization (WHO)2 maintain that healthy people should wear a mask only when caring for a person suspected to be infected with SARS-CoV-2, the virus responsible for COVID-19. The Public Health Agency of Canada (PHAC) similarly does not recommend the use of face masks by healthy people except when caring for the sick, particularly medical masks, but does not discourage the use of non-medical masks by those who wish to wear them, or in situations where physical distancing may be difficult, such as when one is on public transport. PHAC has provided additional advice on the limitations and safe use of masks.
Much of the controversy on mask wearing relates to limited understanding of the transmission pathway for the SARS-CoV-2 virus. Early study of the virus indicates that individual virus particles are approximately 70-90 nm in diameter,4 but virus particles in general are often found clumped together in droplets of fluids or mucous >1 μm.5 Current mitigation strategies for SARS-CoV-2 focus on the main transmission routes via contact and large respiratory droplets (> 5 μm diameter). Less is known about the relative importance of other routes such as aerosol transmission (particles and droplet nuclei < 5 μm diameter).
Most recommendations for population-wide use of masks include the use of either cloth masks or surgical masks, as compared to N95 respirators that are primarily reserved for use in healthcare settings. The function and protective ability vary widely for different mask types. This document outlines the main types of masks, their effectiveness in providing protection against pathogenic hazards, and considerations for the safe use.
Types of masks
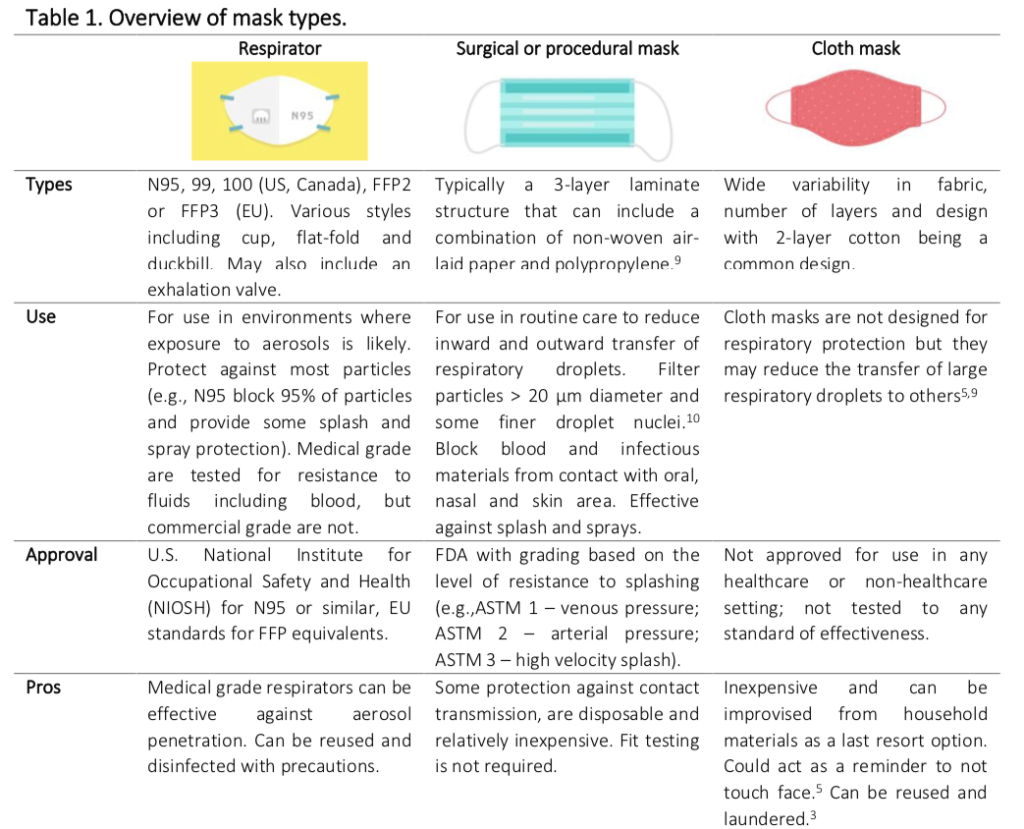
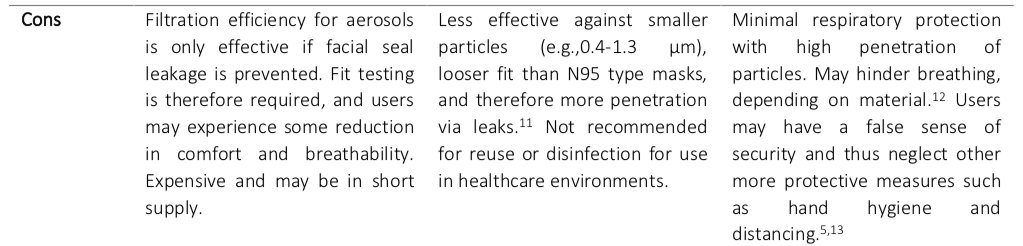
The key groups of masks are medical masks, including respirators (commonly referred to as N95, or filtering facepieces [FFP] masks) and surgical masks, and non-medical masks including homemade cloth masks. Differences between these are summarized in Table 1.
Effectiveness of masks
Masks are worn by individuals either to provide a barrier to the inhalation of particles, or to prevent the exhalation or release of particles due to coughing or sneezing. The effectiveness of a mask is dependent on the level of filtration (determined by the size of particles that can be from seeping around the edges of the mask into the breathing area. Many studies have assessed The effectiveness of a blocked) and the fit of the mask, which can affect the percentage of particles that are prevented the performance of mask types as PPE for protection of the mask wearer, as well as their use by sick individuals for the protection of others. Most studies have been based on generic respiratory viruses and influenza, with only limited study of SARS-CoV-2 published at the time of writing.
Masks as barriers to inhalation of particles
Assessments of the effectiveness of masks to prevent the inhalation of particles have included penetration studies that measure the movement of particles from the external environment through mask material into the breathing zone of the wearer, or studies of protective effect, primarily for healthcare workers (HCWs), that compare clinical outcomes for mask wearers (e.g., incidence of respiratory illness or viral infection) based on different mask-wearing scenarios.
Penetration studies for protection of a mask wearer
Penetration studies that measure the movement of particles from the external environment into the breathing zone behind the mask include those used by agencies such as the National Institute for Occupational Safety and Health (NIOSH) to confirm the protective ability of respirators such as N95s. As expected, the consensus among these studies is that respirators provide superior protection against particles, including aerosols, as compared to either surgical or cloth masks; surgical masks are likewise more protective than cloth masks of all types. N95 or FF2 respirators, when properly fitted, provide a barrier to about 95% of particles. Some studies have found these devices can block in excess of 95%. In similar studies, surgical masks have been found to block about 60% of particles, and may allow penetration by virus particles in high concentration environments, as shown in a study using live influenza virus. Additional PPE such as an integral visor can improve the performance of surgical masks by reducing leakage into the breathing zone around the nose.
Penetration studies of cloth masks find that, in general, they provide a barrier to some larger particles, but performance varies widely depending on the fit and the type of material used. Loose-fitting cloth masks (e.g., handkerchiefs) may provide only minimal protection from inhalation of particles. Masks with conical or tetrahedral shapes that fit closely with face contours perform better than loose-fitting masks. Breathability of fabrics can be a trade-off for filterability. Studies using particles of approximately 20-1000 nm found high penetration levels for cloth masks ranging from 40% (sweatshirt material) to greater than 97% (cotton and gauze handkerchiefs). A study comparing a range of fabrics as barriers to inhalation of microorganisms found that cloth masks allowed for between 30% and 51% of bacteriophage MS2 (as a surrogate for pathogenic viruses) to penetrate the material.12 The study found the most effective cloth material (for breathability and filterability) to be tea-towel material followed by (in order of decreasing effectiveness), a cotton mix, antimicrobial pillowcase, silk, linen, pillowcase, 100% cotton T-shirt, and scarf. None of the fabrics were able to achieve the low level of penetration observed for a surgical mask (11%), which also provided good breathability. Adding multiple layers of the same material appears to provide only limited additional protection, but can reduce breathability.
Protective effect studies assess the effectiveness of masks as barriers to inhalation of infectious particles by measuring the reduced incidence of clinical respiratory illness (CRI), influenza-like illness (ILI) or laboratory-confirmed viral infection among healthcare workers (HCWs) wearing masks versus no masks. In these studies, as expected, respirators are generally found to provide a greater level of protection as compared to surgical masks, with incidence of CRI found to be lower in N95 wearers compared to surgical mask wearers. Further comparison of the incidence of CRI, ILI and viral infections shows a greater incidence of illness among cloth mask wearers compared to surgical mask wearers. Cloth masks are not recommended for health care, or high-risk settlings.
While the protective effect of respirators is difficult to argue, the less protective effect of surgical masks is not always evident. No significant difference in the incidence of laboratory confirmed influenza was found among HCWs at seven US medical centres using N95 respirators versus surgical masks. In a recent case report from China where 41 HCWs were exposed to aerosol- generating procedures for a patient who subsequently tested positive for SARS-CoV-2, none of the HCWs, of whom 85% wore surgical masks and 15% wore respirators, tested positive for SARS- CoV-2. Mask wearing was accompanied by other controls such as hand hygiene and procedural controls. While this is a small case report, and many of the HCWs were exposed only for a matter of minutes, it indicates that surgical masks, when used in conjunction with other measures, can be protective against infection.
Masks as barriers to exhalations of particles
Assessments of the effectiveness of masks to prevent the exhalation of particles have included penetration studies that use coughing tests by healthy or sick individuals to measure movement of particles through mask material to the external environment, or secondary attack rate (SAR) studies that evaluate the effect of mask-wearing by a sick individual in preventing transmission of infection to other individuals living in close contact (e.g., household members).
Penetration studies for protection of others
The effectiveness of masks as barriers to the release of infectious particles can be assessed by measuring the number of microorganisms that can penetrate a mask during exhalation or coughing by the mask wearer. Both surgical masks and cloth masks have been found to block the release of some large droplets but are generally less effective at blocking the release of infectious aerosols. Differences in the effectiveness of masks may depend on the type of virus. One study found that surgical masks reduced the emission of influenza virus in large respiratory droplets, but not in aerosols in exhaled breath and coughs of symptomatic individuals. The same study found that surgical masks blocked the penetration of coronavirus in both large respiratory droplets and aerosols. The only study assessing the penetration of masks by SARS-CoV-2 found that the virus penetrated both cloth masks (2-layer cotton) and surgical masks during coughing by COVID-19 patients.
Secondary attack rate (SAR) studies
In healthcare settings, the use of surgical masks by visitors and healthcare workers has been shown to reduce the incidence of respiratory viral infections among patients. In non-healthcare settings, several studies in France, Germany, Hong Kong, China and Australia have assessed the effectiveness of wearing surgical masks in the home by patients with influenza or ILI to reduce secondary transmission to other members of the household. Some of these studies have found a lower incidence of SAR, but the results did not show statistically significant reductions including one study that assessed the protective effect of both surgical masks and N95 equivalent masks. The greatest reductions in SAR have been observed in studies where mask wearing was implemented early after the onset of symptoms in the sick patient, or where mask wearing was combined with other measures such as hand hygiene.
Considerations for mask use
The hierarchy of controls is used by NIOSH to grade the most effective to the least effective measures for reducing exposures to hazards and is conventionally applied to physical and chemical hazards in the workplace. This framework could be extended to infectious hazards in the general community. Within the framework, the use of PPE is considered a last resort option when other measures have been exhausted. These other measures could include steps to physically eliminate the hazard (e.g., physical isolation), engineering controls to reduce exposure to the hazard (e.g., ventilation) or administrative controls that change the way people work to reduce exposures (e.g., changes to working practices and schedules, hand hygiene). The separation of infected persons from healthy persons, good hygiene practices, cleaning and disinfection of surfaces and engineering controls are known to reduce disease transmission. Following the implementation of these measures, whether masks are used as personal protection for the wearer, or as protection of others from the wearer, there are several considerations that can impact the effectiveness of masks to prevent the spread of viral infection.
Mask fit
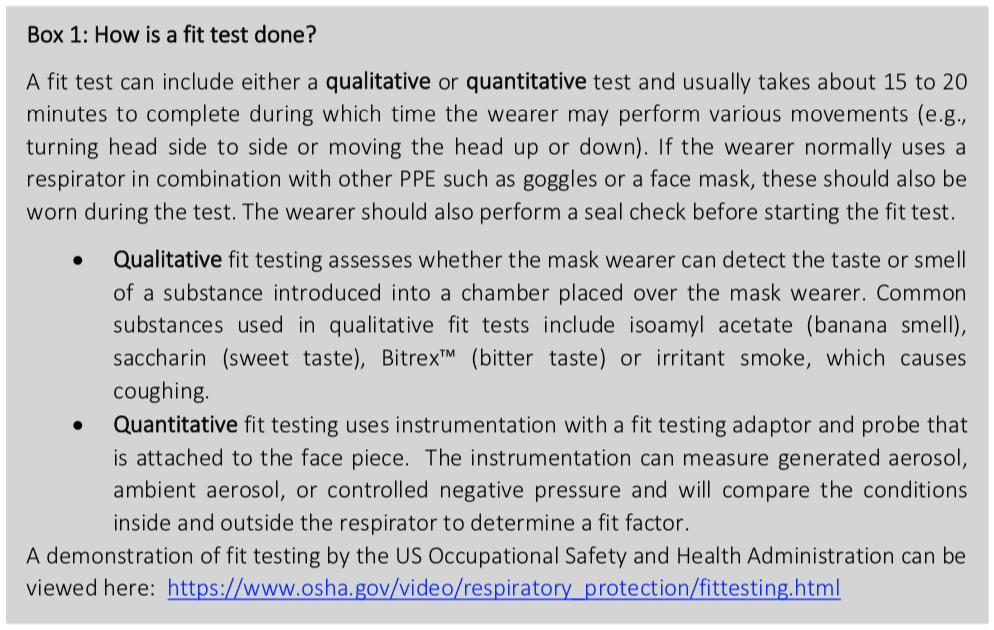
Where respirators are used as PPE, a fit test, and user seal check are essential for ensuring effectiveness of N95 type respirators. Fit tests are used to confirm that a specific make, model and size of respirator provides adequate respiratory protection to the user by providing a tight seal between the facepiece and the face that prevents leakage into or out of the respirator facepiece (Box 1). If the respirator does not pass a fit test, another make, model or size is tested until a suitable respirator is found. The wearer can then use the same make, model, and size of respirator, repeating the test once per year to confirm that fit is maintained, or reconfirming fit if physical changes to the face have occurred, such as weight loss or injury. If the user changes the make, model or size of respirator, a new fit test is required.
A user seal check is different from a fit test and should be performed every time a respirator is put on. Advice on user seal checks is provided by the Canadian Centre for Occupational Health and Safety (CCOHS) and can differ depending on the type of respirator. In general, the wearer identifies a good seal on inhalation by checking that there is slight collapse in the respirator and checks for leakage on exhalation by feeling around the edges or surface of the facepiece. Factors that can influence a poor fit or seal can include damage or deformation of the mask, and the presence of obstructions to fit such as facial hair. For other types of mask, a good fit that aligns to the contours of the face can reduce seepage of air around the edges of the mask. A tight but comfortable fit with effective coverage of the nose and mouth that does not restrict breathability can reduce the frequency that a user touches a mask for readjustment.
Additional PPE
For HCWs or those caring for an infected person, the use of goggles or a face shield that covers the eyes or front and sides of the face, can prevent additional exposures due to splash and spray and block some intake of particles that would occur due to leakage. The appropriate use of gloves (e.g., not touching mask surface, and frequent changing) can also reduce the chance of surface contamination of masks, and similarly washing hands when putting on (donning) and taking off (doffing) PPE, including masks, can reduce contact spread.
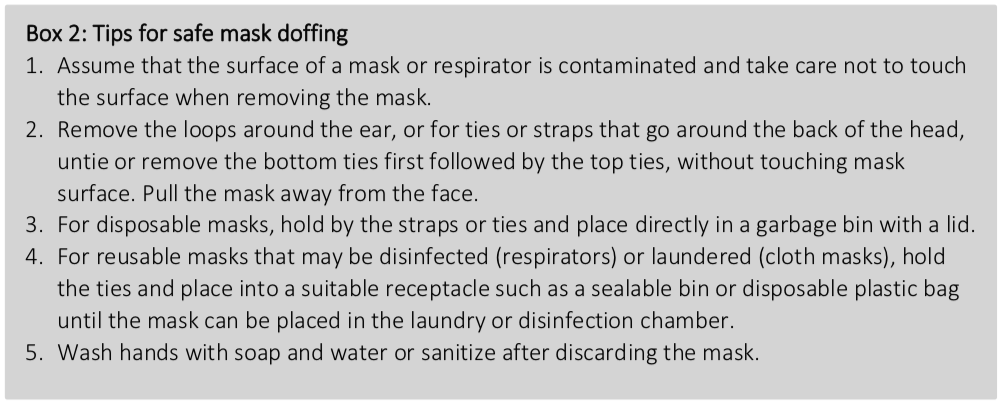
Length of use
The longer a mask is used, the greater the risk for infectious particles to become deposited on the surface. Surgical masks or respirators (e.g., N95) that become wet, damaged, torn, visibly dirty, or contaminated following close contact with an infected person will not provide adequate protection. A study of mask use by HCWs found that very low infection was observed for masks used ≤ 6 hours, however a greater virus positivity was found beyond 6 hours of use, and for HCWs who examined more than 25 patients. The potential presence of viruses on the outer surface suggests a need for caution during doffing practices by avoiding contact with the mask surface (Box 2), and preventing the resuspension of deposited aerosols. Frequent donning and doffing of the same mask can increase the risk of surface contamination on both the inside and the outside of masks and continuous use of respirators may reduce the potential for contamination as compared to frequent donning and doffing of the same mask. In healthcare environments, other measures such as the use of complementary PPE (e.g., face shields) can extend the usability of respirators or masks by reducing the potential for surface deposition or accidental contact with mask surfaces.
Decontamination and reuse of masks
Masks can become contaminated by the user and the external environment. For cloth masks, laundering in a hot wash and thoroughly drying is recommended by PHAC, but any damage, deterioration or reduced fit will reduce the already limited protective function of cloth masks. In general, surgical masks are considered disposable and not recommended for decontamination and reuse. Laundering or disinfection processes can potentially damage the protective layers of the surgical masks, reducing their effectiveness.
Several decontamination methods have been considered for the purpose of providing additional supplies of respirators when there is high demand. The key criteria for effective decontamination methods are stated as: the ability to remove the viral threat, maintaining the integrity of mask elements, and being harmless to the user. Decontamination methods include autoclaving; microwave steam sterilization; washing in soap and water; dry heat treatment; treatment with isopropyl alcohol, bleach, hydrogen peroxide vapour, gamma irradiation; ozone decontamination; UV germicidal irradiation (UVGI) and ethylene oxide treatment. Promising results have been observed for hydrogen peroxide vapour and UVGI; however, any reuse of decontaminated respirators should include steps to inspect respirators for deterioration and damage and to include user seal testing prior to re-use.
Expired masks
Surgical masks and respirators that have been certified by organizations such as NIOSH or the FDA have an expiry date, after which they are no longer considered to be certified. In times of high demand, expired masks may be considered for use following a visual inspection for any damage or degradation of the mask components, including the straps. For expired N95 respirators, the ability to form an effective face seal should also be confirmed by a fit test and user seal check.
Summary
The COVID-19 crisis has resulted in a large upscaling of demand across global health care systems for PPE. Maintaining supplies for healthcare and frontline workers requires judicious use of medical masks including N95 type respirators, which are shown to be the most effective face masks for reducing exposure to viruses for those working in high-risk environments. PPE remains a last line of defence amid other important measures including physical distancing, hygiene and engineering controls.
It is not clear if, or to what extent, the transmission of respiratory viruses is reduced by the population-wide use of face masks, although it is argued by some that the practice during the SARS epidemic in Asia may have provided some protective effect that reduced the transmission of influenza and SARS. In the current COVID-19 pandemic, there is still no firm evidence that the population-wide use of face masks can significantly decrease the risk of infection for healthy individuals or contain community transmission from either infected but asymptomatic persons or from those with symptoms. Further study of the progression of the pandemic in countries that have mandated population-wide use of face masks will help to inform the debate further.
While it has been observed that the use of cloth masks can provide minimal personal protection to the wearer against viral infections, some may argue that some protective effect is better than none. Similarly, the wearing of masks by asymptomatic carriers or symptomatic individuals for the protection of others could be used to reduce the distance a plume of particles generated by a cough or sneeze could travel, similar to common respiratory etiquette recommendations of coughing or sneezing into a tissue or one’s elbow. In most cases, the use of face masks is relatively low risk, and could provide some minimal protection, but if they are used as a substitute for other measures such as maintaining physical distancing and observing good hand hygiene, they could be harmful. They should not be used as a substitute for sick individuals, or those who have returned from travel and may be asymptomatic carriers, to isolate from others Mask wearers should also be aware of the contamination risks from contact with the surface of masks, even when wearing gloves, and considerations for appropriate donning and doffing practices to reduce transfer of contamination.